Inefficient patient flow, delays in admissions, discharge bottlenecks, and underutilised beds is silently costing hospitals between 20% and 30% of potential revenue. This is not a clinical problem. Rather, it is a capacity utilisation problem, and it demands a business transformation strategy.
What Is Patient Flow Inefficiency and Why Does It Cost You Money?
Most healthcare executives track revenue through billing cycles, payer mix, and procedure volumes. In addition, few pause to track the revenue that never gets generated because the right bed, staff, or room was simply not available at the right time.
Patient flow inefficiency refers to any breakdown in the movement of patients through your facility, from admission to discharge, that creates idle capacity, delays care, or forces diversions. Furthermore, the financial consequences are both direct and measurable:
- Ambulance diversions mean lost admissions, typically $1,500 to $3,000 per diverted patient
- Extended length of stay consumes bed capacity that could otherwise serve new patients
- Delayed discharges block downstream admissions in high-demand specialties
- Underutilised surgical theatres and diagnostic units generate fixed costs with no corresponding revenue
- Avoidable readmissions attract penalties under value-based care contracts
For a 300-bed hospital operating at 70% capacity, moving to 82% through smarter flow management can represent millions in incremental annual revenue, without adding a single bed.
How Patient Flow Inefficiency Develops in Healthcare Systems
Understanding the root causes helps decision-makers prioritise where intelligent transformation delivers the fastest financial return. Moreover, addressing these causes systematically is what separates high-performing health systems from those stuck in reactive cycles.
1. Siloed operational data Bed management, nursing schedules, theatre planning, and discharge coordination often run on disconnected systems. As a result, without a unified operational view, bottlenecks are identified reactively rather than proactively, costing time, capacity, and revenue with every delay.
2. Manual discharge planning Discharge decisions are frequently made during morning rounds with no predictive visibility into which patients will be medically ready by afternoon. Consequently, bed turnover is delayed by hours, an effect that compounds across hundreds of beds daily.
3. Demand forecasting gaps Most hospitals cannot accurately predict admission volumes 24 to 72 hours ahead. Therefore, staffing and bed allocation remain reactive, driving both over-staffing costs and under-capacity crisis management simultaneously.
4. Lack of real-time capacity visibility Charge nurses and bed managers typically work from lagging information. Furthermore, by the time a bed is marked available, the next patient is already waiting in ED or recovery, creating a cascading delay effect that ripples across the entire system.
How to Fix Patient Flow Inefficiency Using Intelligent Business Transformation
Resolving this is a structured business transformation challenge, not a clinical protocol change. In fact, the health systems achieving the strongest results are those that treat capacity management as a financial discipline first. Here is how they are approaching it:
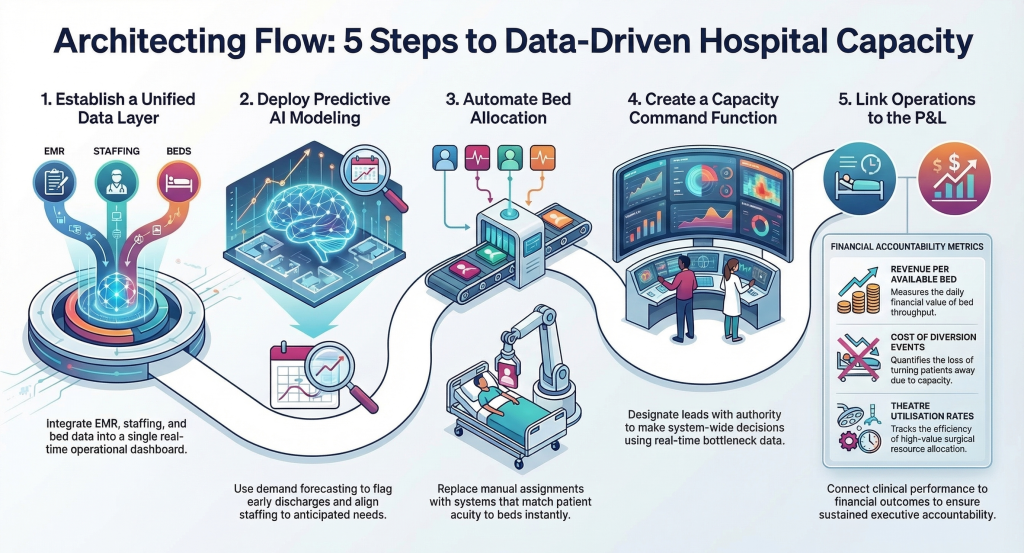
Step 1 : Establish a unified operational data layer Integrate EMR, bed management, scheduling, and staffing data into a single real-time operational dashboard. Doing so removes the blind spots that cause reactive decision-making across departments.
Step 2 : Deploy predictive admission and discharge modelling Use AI-driven demand forecasting to predict patient volumes, flag discharge-ready patients early, and align staffing to anticipated capacity needs, not yesterday’s census. As a result, teams can act on accurate information rather than instinct.
Step 3 : Automate bed allocation workflows Replace manual bed assignment with intelligent systems that match incoming patient acuity to available beds in real time. Consequently, placement delays shrink from hours to minutes, unlocking throughput across the entire facility.
Step 4 : Create a Capacity Command Function Designate operational leads with both authority and real-time data to make system-wide capacity decisions. Additionally, pair this with dashboards that surface bottlenecks before they cascade into system-wide delays.
Step 5 : Measure financial impact, not just clinical metrics Track revenue per available bed per day, cost of diversion events, theatre utilisation rates, and avoidable readmission penalties. Ultimately, connecting operational performance directly to your P&L is what drives sustained executive accountability and long-term improvement.
The Business Case: Capacity Utilisation as a Financial KPI
Healthcare COOs and CFOs increasingly recognise that capacity utilisation belongs in the same conversation as cost per case and payer mix optimisation. Indeed, organisations that treat bed utilisation as a financial KPI consistently outperform those that treat it purely as an operational metric.
Consider these benchmarks:
| Metric | Industry Average | Optimised Systems |
|---|---|---|
| Bed Utilisation | 68–72% | 82–88% |
| ED to Admission Time | 4–6 hours | 90–120 minutes |
| Discharge Before Noon Rate | 15–25% | 40–55% |
| Theatre Utilisation | 70% | 85%+ |
Notably, the gap between average and optimised is not a staffing gap. In contrast, it is a data and decision-making gap, precisely where intelligent business transformation delivers measurable ROI.
Frequently Asked Questions
Q.How does patient flow inefficiency affect hospital revenue?
A. Poor patient flow reduces the number of patients a facility can treat within a given period. Furthermore, fewer admissions, longer stays, and diversions all translate directly to lost billable activity and increased fixed cost per patient.
Q.What technology is used to improve patient flow in hospitals?
A. Solutions typically include AI-powered demand forecasting, real-time bed management platforms, predictive discharge tools, and integrated operational dashboards that connect clinical and administrative data seamlessly.
Q.How long does it take to see financial results from patient flow optimisation?
A. Most health systems report measurable improvements in bed utilisation and length of stay within 60 to 90 days of deploying intelligent capacity management tools. Moreover, revenue impact becomes visible within one to two financial quarters.
Q.What is the role of a COO or CEO in fixing patient flow?
A. Ultimately, executive sponsorship is critical because patient flow optimisation requires cross-departmental authority, capital investment in data infrastructure, and accountability frameworks that link operational metrics to financial outcomes.
The Strategic Imperative
Patient flow is not a ward-level operational problem. Rather, it is a system-wide revenue management challenge that belongs firmly on the executive agenda and treating it as anything less leaves significant recoverable revenue on the table.
At 200OK Solutions, we help healthcare organisations translate operational complexity into measurable business outcomes, connecting the right data, the right processes, and the right technology to unlock capacity that already exists within your system.
Recoverable revenue is already sitting inside your system. Meanwhile, patients need that care today. Bridging the gap, therefore, simply requires the right intelligence layer and the leadership decision to prioritise it.
You may also like: The New Operating Model Healthcare Systems Need to Survive Cost Inflation